If you need help in an emergency or are in crisis visit your local emergency centre or call 911
I am an Employee
Conflict Resolution Process
The Code of Professional Conduct, the Codes of ethics and the Standards of Practice are similar in that they all pertain to governance and regulation of member conduct, while having a slightly different viewpoint in their purpose. Together, the three documents provide a framework for legal and professional accountability for exemplary and responsible practice in all clinical, management, education, and research domains.
The Standards of practice are detailed concepts used to determine what a medical laboratory professional should or should not do. The standards provide a guide to the knowledge, skills, judgment, and attitudes that are needed to demonstrate exemplary competence.
The Code of Professional Conductdescribes the principles, values, standards, and rules of behaviour that guide the decisions and actions of a professional. It is the minimal set of standards for practice that is expected to be upheld within and outside of the professional domain to ensure ‘good standing’ in the profession.
The Code of Ethics includes principles based on an organization’s core values and the standards to which the medical laboratory profession will be held. The Code of Ethics statement provides practical ethical guidance on our ethical values and commitment to providing direct and indirect patient care, working collaboratively with others, the maintenance of our professional identity and our commitment to self-improvement and the improvement of the future workforce.
The Impact of Conflict:
Lost productivity
Poor relationships
Mental health problems
Sabotage
Litigation
Workplace violence and bullying
Absenteeism and / or presenteeism
Employee loss and turnover
Customer loss and impact on sales
There may be a time when someone, or even yourself, may question your ability to uphold the details of these documents. What should you do?
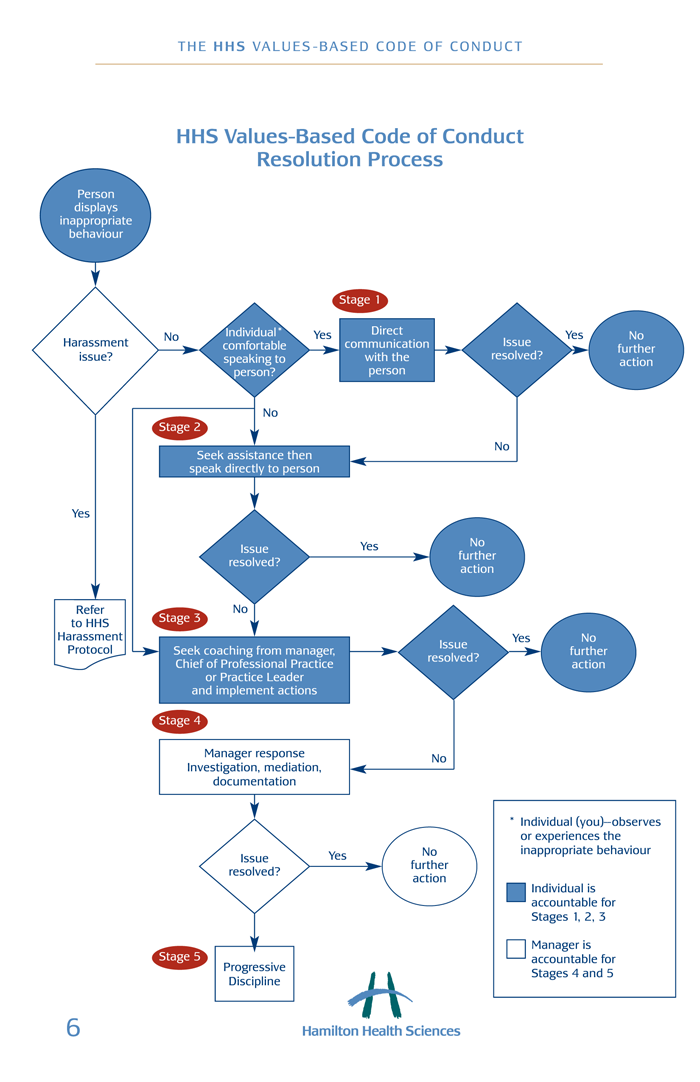
You should start by understanding the general steps behind conflict resolution as defined here.
Get your facts straight! Refresh yourself with the Standards of Practice, Code of Professional Conduct and Code of Ethics to help you identify the core of the issue.
You will also want to seek your local policies and procedures to give you an idea of the resolution process and the requirements of all relevant parties. It is possible that your organization does not have well-documented pathways that are available to you. Firstly, starting with an open dialogue about your concerns with management is a good step.
Start a conversation. This toolkit will provide you with some guidance on how to have a difficult conversation and some useful phrases and words to support your description of the situation. However, none of this information is valuable unless you start the conversation with the right people!
What does the conflict resolution process look like within an organization? See Hamilton Health Science’s resolution pathway below as an example of what one looks like.
Bullying
Bullying does not just happen in the playground with children. It can happen between adults in a formal work environment, between any type of staff (e.g., coworker to coworker, staff to management, management to staff). But how is bullying different from normal conflict that happens? Bullying has been defined as repeated, persistent, continuous behaviour as opposed to a single negative act and is generally associated with a power imbalance between the victim and perpetrator, where the victim feels inferior.
Check twice – Bullying should not be confused with tough management styles. It is different in that it is negative and persistent abuse. Generally, bullying are acts or verbal comments that can “mentally” hurt or isolate a person in the workplace. It is also possible that bullying can be negative physical contact (e.g., pushing, throwing objects).
Bullied employees waste between 10 – 52% of their time at work. Research shows they spend time defending themselves and networking for support, thinking about the situation, being demotivated and stressed, not to mention taking sick leave due to stress-related illnesses.
The following provide examples of workplace bullying behaviours by a man or woman:
Social isolation (silent treatment)
Rumours
Personal attack of a person’s private life and/or personal attributes
Excessive or unjustified criticism
Over-monitoring of work
Verbal aggression
Withholding information
Withholding job responsibility
Trivial fault finding
Replacing proper work with demeaning jobs
Setting unrealistic goals or deadlines
According to the Canada Safety Council, over 80 per cent of bullies are bosses, some are coworkers and a small number of bullies are higher-ups. The Canada Safety Council states that “the target chosen by an adult bully will very often be a capable, dedicated member, well-liked by co-workers. Bullies are most likely to pick on people with an ability to cooperate and a non-confrontational interpersonal style. The bully considers their capability a threat, and determines to cut them down.”
MYTH – People with mental illness are more violent than the rest of the population. In actuality, people with mental illness are 2.5 times more likely to be victims of violence than the general population. See this fact sheet!
There are only a few Canadian jurisdictions that have occupational health and safety legislation specific to bullying. According to the Canadian Centre for Occupational Health and Safety, British Columbia’s WorkSafeBC has developed policies and resources related to workplace bullying and harassment.
All jurisdictions except New Brunswick, Nunavut, Northwest Territories, and Yukon, have legislation about workplace violence and/or harassment. “Where there is no legislation which specifically addressed bullying, the general duty clause establishes the duty of employers to protect employees from risks at work. These risks can include harm from both physical and mental health aspects. In addition, federal and provincial human right laws prohibit harassment related to race, national or ethnic origin, colour, religion, age, sex, marital status, family status, disability, pardoned conviction, or sexual orientation. In certain situations, these laws may apply to bullying.” For up to date information check out their website.
For more resources as an employer or to provide to your organization, look at these comprehensive toolkits for further support:
“Progress is impossible without change, and those who cannot change their minds cannot change anything.” George Bernard Shaw
In a positive trend of results, Bell Canada identified in their 2015 report that:
57% of participants believed that the stigma associated with mental illness has been reduced compared to 5 years ago,
81% were more aware of mental health issues compared to 5 years ago, and
70% believed attitudes about mental health issues have changed for the better compared to 5 years ago.
However, as many know, stigma remains a barrier and there is more we can do to help the fight against it. In fact, there are still many myths floating around that continue the cycle of stigma. Take a moment to read these Top 11 myths about mental illness by Pathstone Mental health.
What is the difference between stigma and discrimination?
We all have attitudes and judgments that affect how we think about and behave toward others. Stigma refers to negative attitudes (prejudice) and negative behaviour (discrimination) toward people with mental health issues or illness.
Stigma includes:
having fixed ideas and judgments—such as thinking that people with mental health issues or illness are ‘not normal’ or ‘not like us’; that they caused their own problems; or that they can simply get over their problems if they want to
fearing and avoiding what we don’t understand—such as excluding people with mental health issues or illness from regular parts of life (for example, from having a job or a safe place to live).
How does stigma cause harm?
One of the biggest hurdles for anyone suffering from mental illness is overcoming the stigma. It is the number one reason why two-thirds of those living with a mental illness do not seek help. According to the Mental Health Commission of Canada, only 23% of Canadians are likely to feel comfortable discussing a mental condition with their employers. That’s not surprising if people with mental health illness also have issues talking directly to their families:
The effect of stigma can be as painful as the impact of mental health issue or illness on a person. Stigma can take many forms but, in the end, the result is always negative. It can cause society to develop the attitudes and actions toward people with mental illness that are harmful:
Fear
Mistrust
Prejudice
Violence
The effect of stigma on people living with mental illness causes them to:
Develop an intense fear of “coming out”
Delay seeking necessary mental health care
Develop a practice of self-stigmatization
Endure discrimination
These displays of discrimination can become internalized, leading to the development of self-stigma: People with mental illness may begin to believe the negative thoughts expressed by others and, in turn, think of themselves as unable to recover, undeserving of care, dangerous, or responsible for their illnesses.
Self-stigma can lead them to feel shame, low self-esteem, and inability to accomplish their goals. It can also lead to the development of the “why try” effect, whereby people believe that they are unable to recover and live normally so “why try”? To avoid being discriminated against, some people may also try to avoid being labeled as “mentally ill” by denying or hiding their problems and refusing to seek out care.
Structural stigma (i.e., stigma that is part of social and institutional policies and practices) presents additional large-scale barriers to mental care by undermining opportunities for people to seek help. A lack of parity between coverage for mental health and other health care, lack of funding for mental health research, and use of mental health history in legal proceedings, such as custody cases, all present structural reasons that people might not seek treatment.
Language is how we express the ideas in our minds and is, therefore, a most powerful agent that can reinforce separation and stigma. However, it can also be used for good. Language can be used to overcome our differences and emphasize the things we have in common. It is beneficial for the medical laboratory community to use common language and shared meaning that reflects and respects the experience of people who live with mental health issues and illness. However, as others have noted before, depending on the local language culture, some terms and definitions may carry different meanings for different people. It is important to take the time and create a mutual understanding of what terms are best and how they are defined.
Think about it for a moment and reflect on the importance of changing our words: People who experience mental health issues or illness may have different perspectives from those of their families and carers. Doctors may see things differently from nurses, social workers or health system administrators. Aboriginal people’s understandings of psychological and social wellbeing may diverge from those of other people born in Canada, or of migrant communities. Those nuances may be contained in a single word or phrase.
Mary Walsh wants to remove damaging labels that lump people together and push them to the side. Watch her video to hear her thoughts. Watch this video:
Many organizations and advocacy groups offer guidelines on dos and don’ts for language but the one component they all agree on is the importance of using “person first” language:
He or she is ‘a person living with depression,’ not ‘a depressive’; a “person with a substance use disorder,” not “an addict.”
Labeling a person using their disability can dehumanize the individual.
Do not use derogatory terms such as insane, crazy/crazed, nuts or deranged. Other recommendations are more subtle such as the word suffering; it is often flagged as presumptive, pitying or fear-mongering. Check out these different resources to support picking the right words.
Victoria Maxwell in her one-woman play “That’s Just Crazy Talk – All Those Crazy Labels” demonstrates all the labels we shouldn’t use. You’ll get the point in a not so serious way! Previous research has demonstrated that the live stage play was effective in reducing stigma and that the recorded version may also be effective as an anti-stigma tool.
Also, check with your organization to find out if a language policy exists in your workplace. At the very least, simply ask the person you are speaking with which term he or she prefers or if your language choice is appropriate. It’s perfectly ok to admit that you want to learn. In fact, it’s the right thing to do.
How to Change Stigma?
“I know that every time I talk about this and someone listens, someone’s life is changed.” ~ Michael Landsberg. Watch his testimonial and hear about a moment that changed his life:
Adopted from the Shatter The Stigma Mend The Mind campaign, here are seven important things we can do to reduce stigma and discrimination:
1. Know the facts.
Educate yourself about mental health issues and illness. Learn the facts instead of the myths. Visiting our website is a great place to start!
We’ve all grown up with prejudices and judgmental thinking. But we can change the way we think! See people as unique human beings, not as labels or stereotypes. See the person beyond their mental illness; they have many other personal attributes that do not disappear just because they also have a mental illness.
The way we speak can affect the way other people think and speak. Don’t use hurtful or derogatory language.
See the Mental Health Toolkit links in the “Language Matters” section!
4. Educate Others
Find opportunities to pass on facts and positive attitudes about people with mental health issues and illness. If your friends, family, co-workers or even the media present information that is not true, challenge their myths and stereotypes. Let them know how their negative words and incorrect descriptions affect people by keeping alive the false ideas.
People with mental health issues and illness make valuable contributions to society and medical laboratory profession. Their health problems are just one part of who they are. We’ve all heard the negative stories. Let’s recognize and applaud the positive ones.
Treat people who have mental health problems with dignity and respect. Think about how you’d like others to act toward you if you were in the same situation. If you have family members, friends or co-workers with substance use or mental health problems, support their choices and encourage their efforts to get well.
7. Include everyone
In Canada, it is against the law for employers and people who provide services to discriminate against people with mental health and substance use problems. Denying people access to things such as jobs, housing and health care, which the rest of us take for granted, violates human rights.
People with mental health issues and illness have a right to take an equal part in society. Let’s make sure that happens.



 There may be a time when someone, or even yourself, may question your ability to uphold the details of these documents. What should you do?
There may be a time when someone, or even yourself, may question your ability to uphold the details of these documents. What should you do?